3/8
The one thing that I do notice, still, is the correlation between the amount of fluid under my scalp and my functionality. There’s definitely more fluid back there and more headache and more impairment when weather’s coming in – I know you have the weather predicting sinuses, too, so you know what I mean. I don’t know whether sinus swelling pushes cerebrospinal fluid out of my skull and into my balloon scalp, but it certainly seems like it.
Rarely, I’ll find myself experiencing balance or spatial relations or aphasia issues without the increase in fluid, but most often the two things happen at the same time.
3/11
There is a huge amount of frustration involved in the length of this recovery and the limits it imposes. Today is five months from my surgery, and my scalp is so full of fluid that the tops and backs of my ears are numb; the pressure from the fluid in my neck is uncomfortable when it’s not painful, and makes my throat sore; feeling exhausted is the norm, even when I’ve slept 12-14 hours; I still get intermittent aphasia and loss of balance and disorientation.
Don’t get me wrong – things are better. They’re just not all better, and they’re not consistently or predictably better. The night of my last update, we were watching television, and the host said the phrase, “Where’s the beef?” The name “Clara Peller” popped right into my head, and I remembered the story behind it completely. The very next night, I was asking DH to go with me to Costco because I was having some anxiety about the overstimulation for some very specific reasons that I’d already been thinking about during the day. Then I lost the words. The nouns, in particular, and even though I know now that there were other words I could have used that were different parts of speech as substitutes, I couldn’t mentally get past the lost words. Because they were lost, there was apparently no way to find the substitutes, because they were associated with the words I couldn’t find. Of course we’re in public, of course I’m fighting back tears, and of course it’s the first time I’ve worn makeup in ages, and of course I smeared it wiping tears away. That’s a truly minor thing, but at the moment it was the icing on the cake.
My antidepressant is working. The tiny bit of Adderall I’ve started on is helping. I’m cutting back slowly on my alprazolam. The problem I’m battling now is not something medications can fix. Anyone who says “Gee, I wish my doctor would prescribe months of bed rest” is going to get smacked in the head. Hard.
3/15
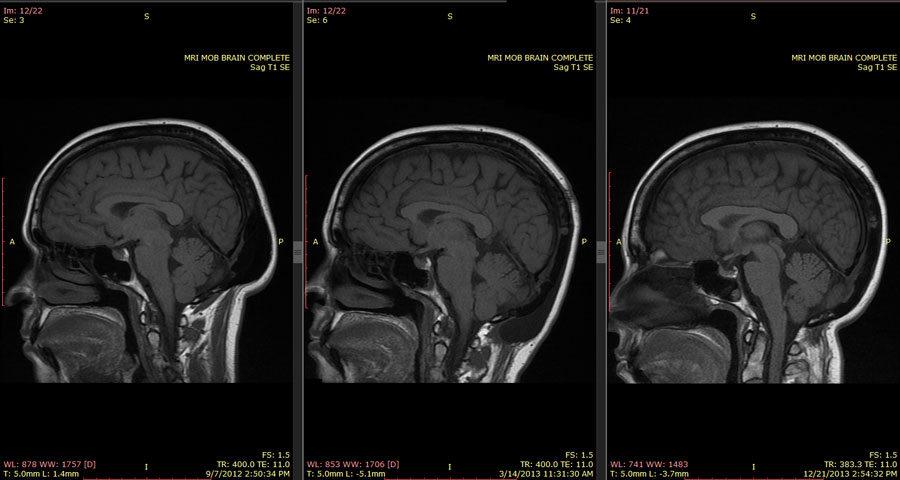
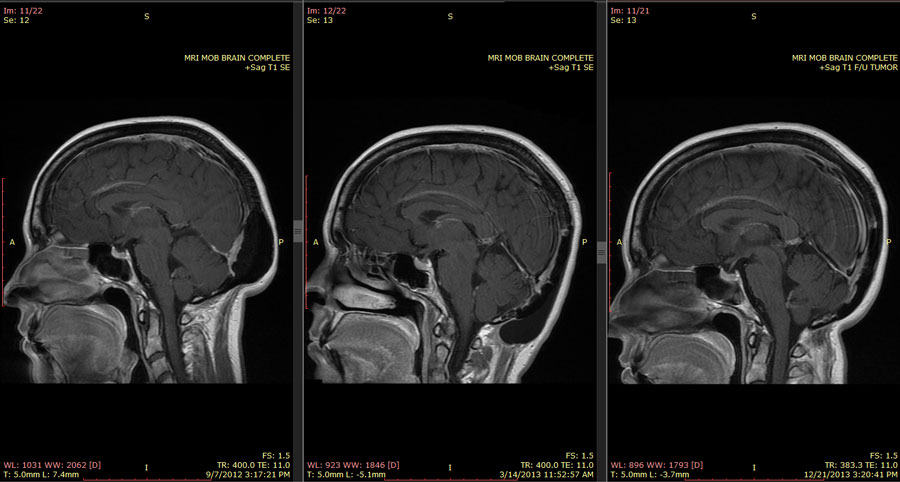
The MRI was. . .interesting. My left hemisphere has clearly stretched itself back out quite a bit, but you can see that the gyri and sulci (the folds and bumps of the brain, respectively) are distorted, and there’s something that looks like fluid accumulation between them in certain areas. My left frontal lobe is swollen or distorted or pushed somehow by fluid, and you can see that it is pushing on my right frontal lobe by the curve in the gap between the hemispheres.
My occipital lobes seem to be quite happy with their new freedom, as my visual perception seems to be working just fine. It’s my left eye itself that’s affected, and I’m wagering that it’s because of the pressure from whatever it is that’s distorting my left hemisphere.
My short-term memory has really taken a hit, but I can remember things when I’m reminded of them. This is an improvement over not being able to recall things at all, but it’s still frustrating to not be able to retain them voluntarily.
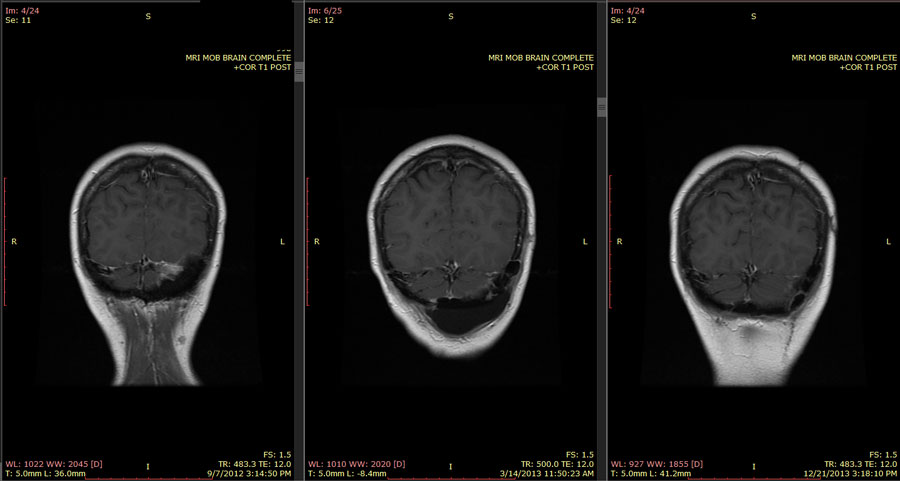
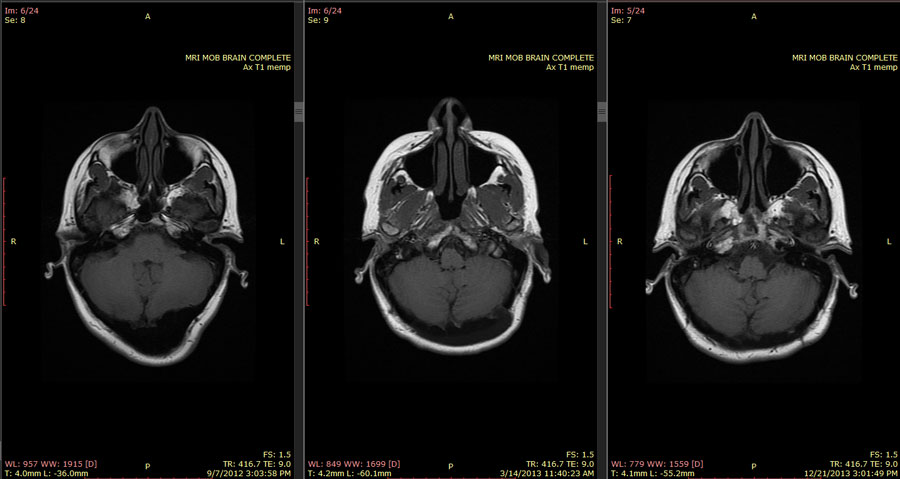
Looking at the MRI itself gave me a reference point for the improvement in my spatial relations – before surgery, looking at the scans, it was nearly impossible to orient myself as to what was where. When you look at these scans, it is as if you were looking at another person, with left and right reversed. Before surgery, I couldn’t get beyond the perception that it should have been a mirror image. The axial (horizontal) scans start from bottom to top, and the saggital (back to front, like an arrow shot by saggitarius!) scans go from left to right, and the coronal (side to side, like a crown!) scans go from back to front. I started off looking at this second set having the same difficulty grasping that as I had before, but slowly began to be able to put left and right, front and back, and bottom and top in their correct relative places.
I have to figure out how to compare the before and after shots side by side, but I’m not in a rush to do that right now. The neurosurgeon will have better insight on that come Tuesday.
3/19
Well, I’ll be going off to the hospital again. And my hair was growing in so nicely, too! My brain looks good, according to the neurosurgeon, but I sprung a leak between the bone and the new and improved plastic skull assembly. That needs to be looked at and patched, and I need a shunt to siphon off all the cerebrospinal fluid that’s in my neck and under my scalp. It’s not going to go away by itself, and it’s the reason I’m in pain.
The only bad news is really that the pain level for the first week of recovery is going to be pretty bad – but that’s better than living with what I’m feeling now for the rest of my life. The surgery itself is pretty simple for this doctor, and will take less than 2 hours. And he made a note that I don’t respond to morphine, so I’m actually a lot less concerned about the pain, anyway.
The adventure never stops. . .
SURGERY UPDATE
The Hospital
I got lucky; the first patient of the day cancelled, so I got in before I really had a chance to think about how hungry I was or how much I wished I had gotten a cup of coffee. All the preadmission questionnaires and consults with the assisting physicians and getting IV hookups took about an hour, but it wasn’t long before I was being wheeled into the OR and getting an armful of Versed, which would make me forget everything that happened after they attached the safety straps that would allow them to turn me face down.
Recovery
I didn’t stay long in recovery, but I could tell right from the start that this thing was going to hurt like anything. They had drained pretty close to a pint of fluid from under my scalp and the back of my neck. In order to press the scalp against my skull, prevent further fluid accumulation, and hold the patch in tight to the bone, they had packed a good couple of inches of gauze rolls against the incision/drained area and then wrapped me in a massively tight turban of more gauze and tape. As soon as my surgeon had seen me, explained how they had ended up doing the procedure, and what I was in for in the ICU, I was rolled up there.
ICU
The original plan was to drain 10cc per hour of cerebrospinal fluid through the lumbar drain that had been inserted into my spine. My surgeon was on call, and supervised the first drain. After 3ccs, it felt like a few dozen ice picks had been plunged into my skull all at once. So, new plan of action was to stick with 5ccs per hour, and to drain as slowly as possible. My first two ICU nurses were kind, caring, gentle people who treated me very well. . .day 2 in ICU was pretty unbearable.
Keep in mind here that I’m on a heavy duty opiate for pain, and it kind of sort of takes a little of the edge off. Keep in mind that after a lumbar drain, my pain is so huge that it no longer has an edge. Daytime ICU nursing staff really didn’t consider this much of an issue. In fact, the common procedure was for the alarms and call bells to go unanswered while the nurses talked about the houses they were buying, how many of each kind of baby they wanted, and food.
My IV alarm went off multiple times, and I always pressed the call button, because usually all it needed was to be reset. If I pressed that call button and saw a nurse in less than a half hour, it was a miracle. In fact, I could press that button and see her looking into my room, and she would either continue eating, or walk around to the other side of the nurses’ station. So just for ha-has, I didn’t press the call button – until my IV alarm had beeped 400 times and I was getting tired of listening to it. They would also start my lumbar drain and then leave – and the idea of having more than 5ccs taken out while they disappeared for a half hour or so was pretty frightening to me.
Therefore, it was no surprise that this nurse decided on my second full day in ICU that it was about time I sat in a chair. Immediately after my lumbar drip was done and my head was exploding. Adding insult to injury, I still had a foley in, and she hooked the bag right on my pulse ox wire so my left hand was trapped. I started yelling that I was going to pass out, because, of course, they left me alone in the room like this, and they came in and saw me white as a sheet and drenched in sweat so bad that the dressing holding the lumbar drain came loose and decided maybe it wasn’t quite such a good idea to make me sit up after all. The fact that for a half hour or so after that my pulse kept dipping down into the low 40s and they had to call in my surgeon kind of made it clear this wasn’t something to try again.
The trip down to get a CAT scan was a pretty unpleasant adventure, as well. Hey, guys, that’s a conscious, living human being on that bed who’s just been through major surgery. Do not ride my bed down the ramps and swing me 90 degrees to the left just before we hit the wall, and then whip me around 90 degrees to the right to go through the next door. I am really not here for an amusement park experience. And maybe you could talk to me instead of carrying on a personal conversation between each other, you know, as if you’re concerned about my health and well-being.
The other unpleasant thing was a matter of dignity. This surgery made it so that even the slightest change in orientation from horizontal was excruciating. The pain from the incision and the packing in my neck hurt the back of my head, and the decreased fluid cushion around my brain gave me the stabbing headache in the front. However, at some point, they need to take the catheter out and you have to use a bedpan. My one good ICU nurse was joined by another good one on my last day, and both of them understood that going in a bedpan requires more cleanup than using a toilet – and both of them gently helped me turn over and lower the head of the bed and take care of that, because I couldn’t do it myself. One other nurse didn’t clean up my back and thighs, but at least she changed the pad. The others from the infamous day shift left me minimally wiped, and lying on a urine-soaked pad, which eventually soaked up into my gown, as well.
Upstairs to the regular rooms
This really is a different experience. It also helped that some of the nurses, food service, and cleaning staff remembered me from last time – they treated me wonderfully then, they treated me wonderfully this time. I was there Monday and Tuesday and part of Wednesday, and I didn’t have to worry about my pain being ignored, or not being able to get help to get to the bathroom on time, or my doctor not being called when his directions were needed.
The procedure
So, the surgical cement that had been used to replace the bone that had been removed in my original surgery was fine, but my own bone simply didn’t knit with it in one specific spot. I had been experiencing a pretty marvelous recovery, but then all of a sudden, my scalp started to fill up with more fluid, instead of continuing to flatten out as it had. Then the headaches started, in my forehead and slightly upwards, perfectly symmetrical, and with a distinct margin between pain and no pain. I could have drawn these headaches on my head with a sharpie.
The MRIs showed exactly where the fluid was leaking and where it was accumulating. This meant opening up an incision as close as safely possible to the hole, draining out the fluid that had escaped into my scalp and neck, sealing the hole with the same surgical cement, then using a combination of pressure dressings on the outside and draining cerebrospinal fluid from the inside to keep the new patch securely in place while it cured.
After, the headaches were the same as before, only much, much more intense. My surgeon says that these symmetrical headaches that start around eyebrow level and move upwards are pretty typical of low pressure headaches, and there are investigations going on to see if there’s a connection between “weather headaches,” which have most of the same qualities, and an actual drop in CSF pressure.
Once I got home, I discovered quite by accident that the horrible pain (yes, it was still horrible. Really, really horrible) that hit the moment I started to get vertical, and which became worse the longer I stayed upright, could be mitigated by holding my hands over my head. I will try this trick for other headaches, you can be sure. The only thing that makes the headaches bearable is being horizontal. However, the pain medications are much more effective today than they were even yesterday. Staying horizontal as much as possible is essential to my recovery so that pressure inside my skull doesn’t fluctuate more than necessary.
The weird stuff
So, as I remember, I’m going to try to pass on some information about my experiences. Some things are unique to me, but some are common in brain injury that includes loss of cerebrospinal fluid.
Day one, my dreams were frenetic and without plot or direction. If you’ve ever seen a movie or TV show in which a character is being filled with information from a computer, and it’s just screen after screen of images and characters in rapid succession, that was what I was dreaming. None of it made sense, and there were more images of white screens full of alphanumeric text than anything else. I felt emotionally disturbed by these dreams, even though there was nothing inherently frightening about them. There has been a slow transition between dreams that consist solely of flashing images to normal dreams that are momentarily interspersed with these images.
This could be from the physical trauma of surgery, loss of CSF, or a side effect of the medications. It could also derive in part from the fact that I was being awakened at least once an hour, so it made me remember the dreams more!
Sound and light bothered me, just as they would if I were having a migraine headache. Draining the fluid cushion added another dimension – all the sounds around me seemed to be coming through a drum with a clear plastic head. (Drummers, you know what I’m talking about – it’s a very specific type of reverberation.) The lower the pitch, the more reverberation, and the more painful it was to hear. My surgeon and his PA confirmed that this was related to fluid levels, because it changed how much my eardrums vibrated.
I often felt as if my head and my body were somewhat separated. After the nausea dissipated, I felt perfectly normal from the neck down, restless and ready to get up and move around. When I did, though, it felt almost as if my head were moving through thicker air than the rest of me.
That’s all that comes to mind right now, but I’ll add more as I remember it.